About 'Bling-k Of An Eye'
I began making sparkly eyepatches after losing my eye to a very rare type of cancer in my tear gland. I found it difficult to find attractive eyepatches so I started to customise my own.
After support from my medical professionals, I decided to make 'bling-k of an eye' to help others in a similar situation to myself and to raise awareness of adenocarcinoma of lacrimal gland. I recommend speaking with a medical professional before using an eye patch and they shouldn't be worn as a replacement for any dressings or bandages, just to cover them up and help people feel more confident when having to wear an eyepatch.
After support from my medical professionals, I decided to make 'bling-k of an eye' to help others in a similar situation to myself and to raise awareness of adenocarcinoma of lacrimal gland. I recommend speaking with a medical professional before using an eye patch and they shouldn't be worn as a replacement for any dressings or bandages, just to cover them up and help people feel more confident when having to wear an eyepatch.

The night before my biopsy
Back in 2016 I was diagnosed with cancer in my tear gland.
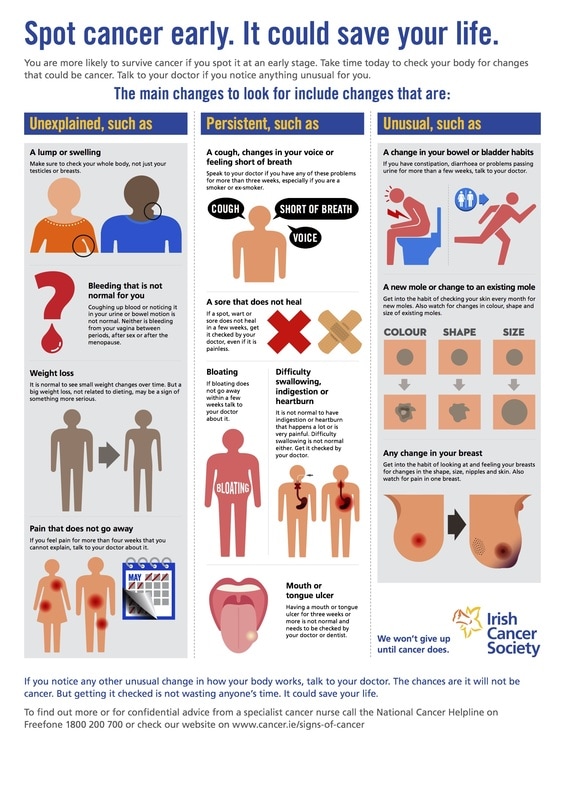
The first thing I noticed physically was the swelling around my eye, this grew very quickly and I was noticing a change in size everyday. It was pushing my eye forward and this resulted in puffiness and swelling. I also had a lot of pain in my head and eye.
I had double and blurred vision and when I moved my eye it jumped rather than move smoothly. I was also very tired and felt generally unwell. When I visited my opticians they said my macular at the back of my eye was striped, where it had been folded down by the tumour.
It was this that prompted an MRI scan which showed a lesion in my tear gland. I was sent to Moorfields eye hospital in London for a biopsy, I was also given many other tests to try and find the cause of these symptoms.
A week later I was diagnosed with adenocarcinoma in my tear gland, my doctors said it was very aggressive and extremely rare. I had a full body scan to check the cancer hadn't spread, luckily it was all contained with the gland.
As this cancer was so aggressive and chemotherapy resistant I had to have my eye and eyelids removed for my best chance of survival, an orbital exenteration. In September 2016 I had a 6 hour surgery at William Harvey Hospital in Ashford to remove my eye, everything went well and a few weeks later I was told I had clear margins, so didn't need any further treatment.
I was so thankful and thought this was the end, however after almost two years I started getting pain around the area where my eye used to be, after speaking with my surgeon, it was agreed that I should have an MRI to find out what was causing the severe pain. When the results came back it was confirmed, there was a lump in my eye socket. I was immediately sent for a biopsy and a week later, 19th November 2018, I was diagnosed with a reoccurrence of adenocarcinoma. No-one understood how it had returned but it was decided that I would need another operation, thus time I would need to travel to London for the surgery as a neurosurgeon needed to perform the operation.
On the 29th January 2019 I was in London Charing Cross hospital for the 5 hour surgery. The surgeons cut across my head from ear to ear to remove the tumour and surrounding bone and move some facial muscles with minimal scarring and I also had a skin graft from my thigh. I was in London for 5 days and although I came out of surgery feeling much better, my hair wasn't in the best condition, this was when I had the idea of 'braving the shave' for Cancer research UK. I set up the fundraising page from my hospital bed and by the time I returned home I was pleasantly surprised with the donations. I decided to keep my fundraiser open until the end of the radiotherapy treatment and raised over £1000 plus gift aid, by the time i had finished 6 weeks of radiotherapy.
After my first surgery I started making customised eyepatches and I still enjoy to make these for other people as well as myself. My page is Bling-k of an eye and I sell these patches to other people who are in need.
The first thing I noticed physically was the swelling around my eye, this grew very quickly and I was noticing a change in size everyday. It was pushing my eye forward and this resulted in puffiness and swelling. I also had a lot of pain in my head and eye.
I had double and blurred vision and when I moved my eye it jumped rather than move smoothly. I was also very tired and felt generally unwell. When I visited my opticians they said my macular at the back of my eye was striped, where it had been folded down by the tumour.
It was this that prompted an MRI scan which showed a lesion in my tear gland. I was sent to Moorfields eye hospital in London for a biopsy, I was also given many other tests to try and find the cause of these symptoms.
A week later I was diagnosed with adenocarcinoma in my tear gland, my doctors said it was very aggressive and extremely rare. I had a full body scan to check the cancer hadn't spread, luckily it was all contained with the gland.
As this cancer was so aggressive and chemotherapy resistant I had to have my eye and eyelids removed for my best chance of survival, an orbital exenteration. In September 2016 I had a 6 hour surgery at William Harvey Hospital in Ashford to remove my eye, everything went well and a few weeks later I was told I had clear margins, so didn't need any further treatment.
I was so thankful and thought this was the end, however after almost two years I started getting pain around the area where my eye used to be, after speaking with my surgeon, it was agreed that I should have an MRI to find out what was causing the severe pain. When the results came back it was confirmed, there was a lump in my eye socket. I was immediately sent for a biopsy and a week later, 19th November 2018, I was diagnosed with a reoccurrence of adenocarcinoma. No-one understood how it had returned but it was decided that I would need another operation, thus time I would need to travel to London for the surgery as a neurosurgeon needed to perform the operation.
On the 29th January 2019 I was in London Charing Cross hospital for the 5 hour surgery. The surgeons cut across my head from ear to ear to remove the tumour and surrounding bone and move some facial muscles with minimal scarring and I also had a skin graft from my thigh. I was in London for 5 days and although I came out of surgery feeling much better, my hair wasn't in the best condition, this was when I had the idea of 'braving the shave' for Cancer research UK. I set up the fundraising page from my hospital bed and by the time I returned home I was pleasantly surprised with the donations. I decided to keep my fundraiser open until the end of the radiotherapy treatment and raised over £1000 plus gift aid, by the time i had finished 6 weeks of radiotherapy.
After my first surgery I started making customised eyepatches and I still enjoy to make these for other people as well as myself. My page is Bling-k of an eye and I sell these patches to other people who are in need.

The day after my orbital exenteration.
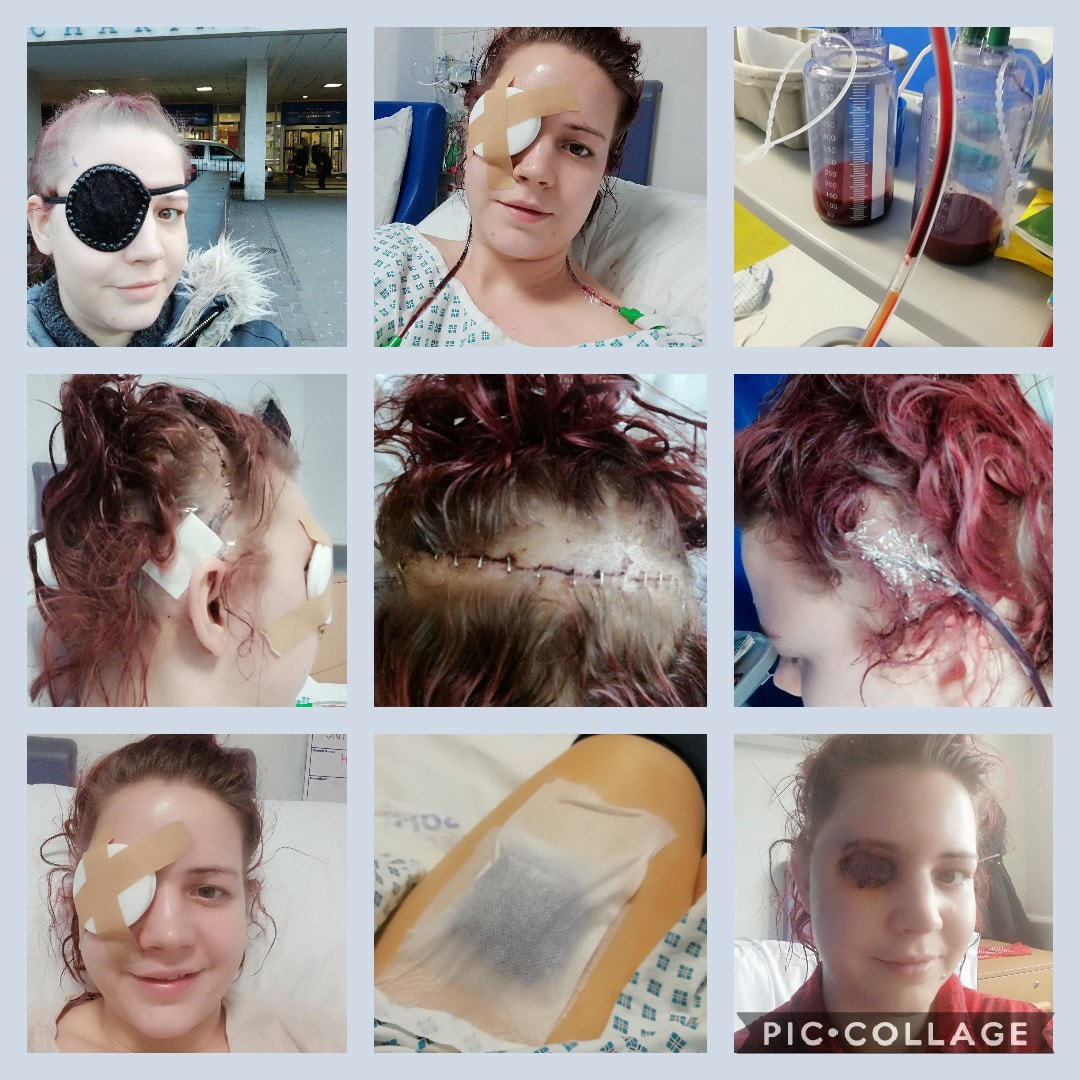
Pictures from my 2nd surgery in 2019
🎗ADENOCARCINOMA OF THE LACRIMAL GLAND. It is very difficult to find information online so I am sharing this to hopefully raise awareness. 🎗
Tumors of the lacrimal gland represent 10 percent of all mass occupying lesions in the orbit and are broadly classified as epithelial and non-epithelial lesions. Traditionally, it has been said that 50 percent of the lacrimal masses are epithelial and 50 percent are non-epithelial. However, more recent data indicate that non-epithelial tumors account for 80 percent of the total of the lacrimal gland tumors (this includes inflammatory and lymphoid lesions).
Of all orbital lesions, lacrimal epithelial tumors comprise from 5 to 8 percent, with half of these being benign mixed tumors and the other half carcinomas.
Adenocarcinoma comprises 7 percent of the epithelial tumors of the lacrimal gland. It affects older patients (18 to 80, mean 58 years) and is more common in the male population. Clinical presentation is that of a rapidly growing and palpable mass that causes proptosis, globe displacement, diplopia, ptosis, visual loss and pain.This tumor has a more aggressive behavior and a shorter patient survival time than adenoid cystic carcinoma (1.5 years). Mortality is associated with an early lymphatic dissemination of the tumor cells to lymph nodes and lungs. Aggressive treatment is warranted, including a monobloc craniofacial orbitotectomy, exenteration, lymph node dissection and subsequent radiotherapy. Patients under this protocol have shown a better survival rate and fewer recurrences.INFORMATION FROM MACMILLAN WHEN I PHONED FOR ADVICE.
Tumors of the lacrimal gland represent 10 percent of all mass occupying lesions in the orbit and are broadly classified as epithelial and non-epithelial lesions. Traditionally, it has been said that 50 percent of the lacrimal masses are epithelial and 50 percent are non-epithelial. However, more recent data indicate that non-epithelial tumors account for 80 percent of the total of the lacrimal gland tumors (this includes inflammatory and lymphoid lesions).
Of all orbital lesions, lacrimal epithelial tumors comprise from 5 to 8 percent, with half of these being benign mixed tumors and the other half carcinomas.
Adenocarcinoma comprises 7 percent of the epithelial tumors of the lacrimal gland. It affects older patients (18 to 80, mean 58 years) and is more common in the male population. Clinical presentation is that of a rapidly growing and palpable mass that causes proptosis, globe displacement, diplopia, ptosis, visual loss and pain.This tumor has a more aggressive behavior and a shorter patient survival time than adenoid cystic carcinoma (1.5 years). Mortality is associated with an early lymphatic dissemination of the tumor cells to lymph nodes and lungs. Aggressive treatment is warranted, including a monobloc craniofacial orbitotectomy, exenteration, lymph node dissection and subsequent radiotherapy. Patients under this protocol have shown a better survival rate and fewer recurrences.INFORMATION FROM MACMILLAN WHEN I PHONED FOR ADVICE.